Chamber III
Pulse.
Three fingers. Three positions. Three depths. That is the alphabet.
Chamber III
Three fingers. Three positions. Three depths. That is the alphabet.
The pulse is not a number. It is a piece of music. Western pulse-taking measures one thing — beats per minute. Classical pulse-taking reads a textured field: rate and rhythm, yes, but also depth, force, shape, quality, and the comparison between the left wrist and the right.
The reframe matters. A number can be in range or out of range. A piece of music can be in tune or out of tune — but the question it asks is richer, and the answer it carries is deeper. Sixty-eight beats per minute tells you one thing. A wiry, rapid pulse on the left guan tells you something else entirely.
Put your fingers on what's real.
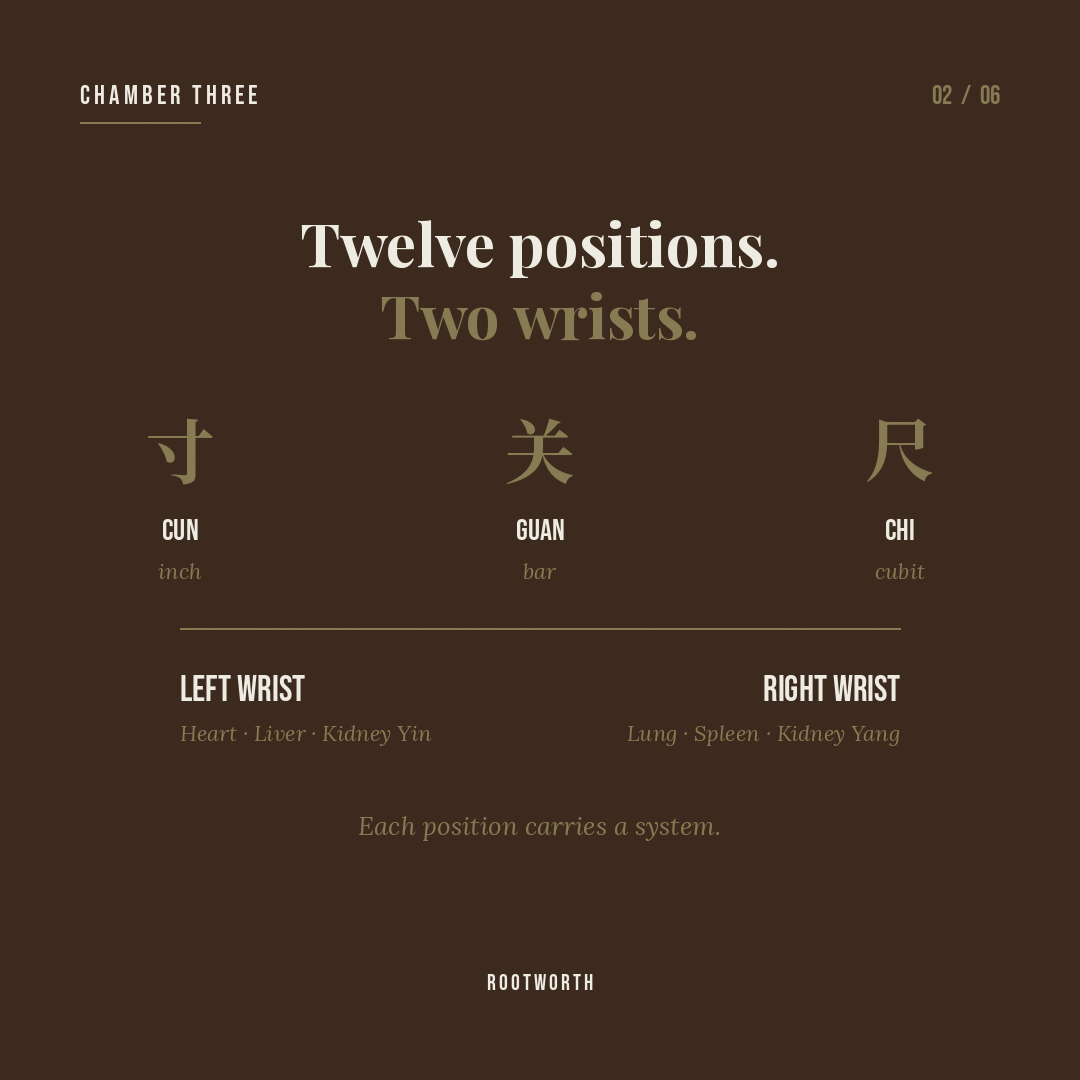
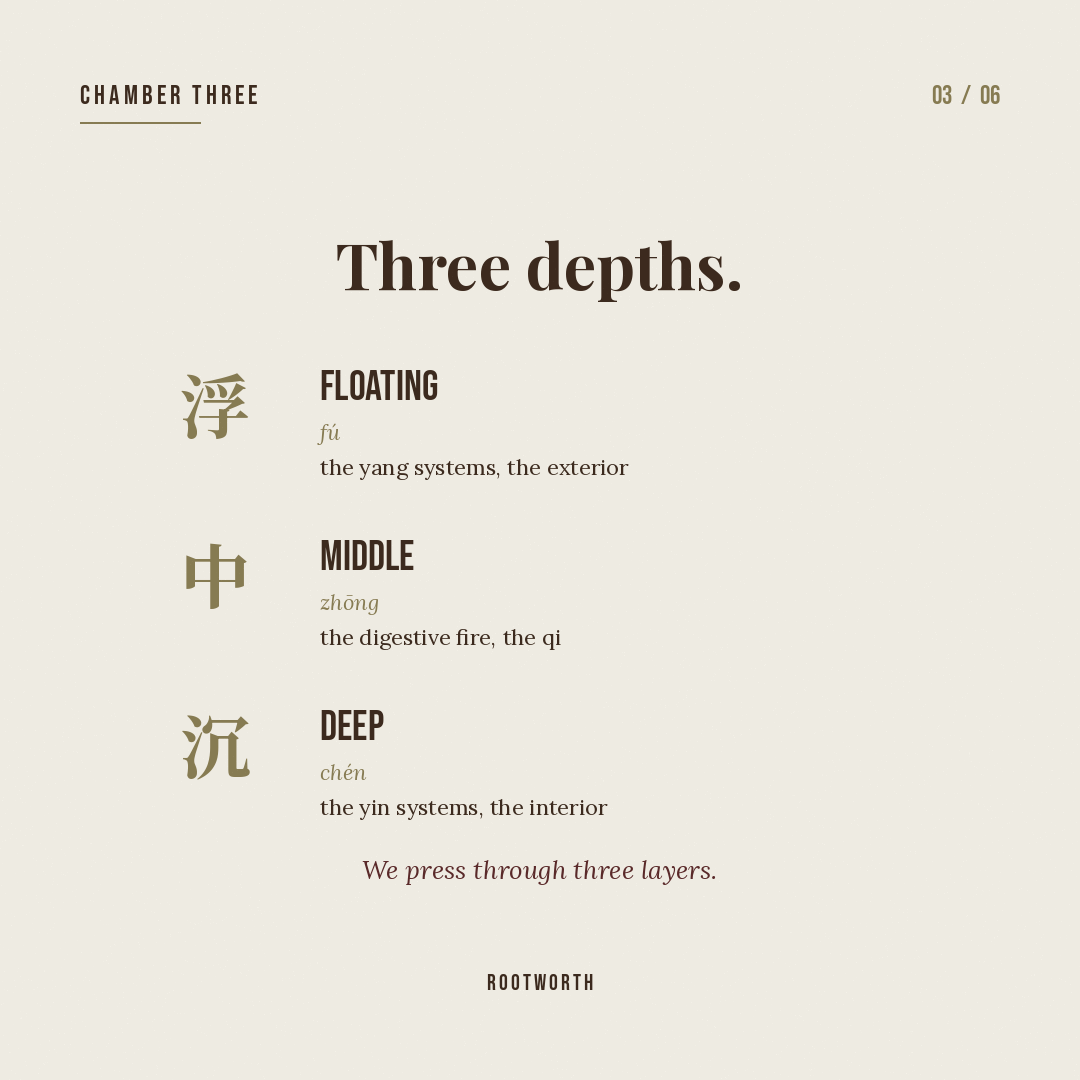
The practitioner places three fingers on the radial artery, at three positions — proximal, middle, distal — and at three depths — superficial, middle, deep. That is nine readings per wrist. Eighteen across both. Each reading is a window onto a specific organ pair and a specific quality of qi and blood.
The left wrist reads the Heart, Liver, and Kidney. The right reads the Lung, Spleen, and Kidney gate. The comparison between sides is itself information. A strong pulse on the left and a weak one on the right is a different picture than the reverse — even if the individual positions look similar on their own.
Long before the patient describes their symptoms, the pulse has already named the pattern. A slippery pulse on the right middle position says damp in the spleen. A wiry pulse on the left guan says liver qi stagnation. A thready pulse at depth says blood deficiency.
What the pulse cannot say, the tongue and the intake will. What the patient cannot say, the pulse often does. A skilled practitioner reading the pulse is not guessing — they are reading a clinical language that has been refined over two thousand years of daily practice, in hundreds of thousands of patient encounters, tested against outcomes and refined by masters who left the receipts.

The 28 named pulse qualities — slippery, wiry, thready, tight, deep, floating, rapid, slow, intermittent, hidden, scattered, and on — are a working language, not metaphor. Each one names a specific texture of movement. Each one corresponds to a specific pattern in the body.
A slippery pulse moves like pearls rolling on a plate. A wiry pulse resists the finger like a taut guitar string. A scattered pulse is wide and soft and loses definition under pressure. These descriptions are not poetic. They are clinical discriminators that tell the practitioner where to look next.
The classical pulse is a four-dimensional object: rate, depth, width, and quality. These four, read at eighteen positions, are held together in a single integrated picture. No single position is the diagnosis. No single quality is the diagnosis. The pattern that emerges from the full reading — held with the tongue and the intake — is what the practitioner treats.
Modern medicine has begun to arrive at this. Heart rate variability research reads the rhythm in a way classical practice has always read it — not for a number, but for what the rhythm is doing across time. The instruments are newer. The reading is not.
The pulse is where the practitioner stops listening to language and starts listening to the body. It is the moment the intake becomes diagnosis. The pattern that emerges from eighteen positions, compared with the tongue and the intake, is not an average — it is a picture of how this person's body is responding to its conditions right now. That picture is what the formula answers.
Modern medicine measures blood pressure. We read what the blood is saying.
Chamber V continues this thread — the pulse is music, and the body keeps a beat. If pulse is the alphabet, the rhythms in Chamber V are how the alphabet becomes language.